
- GLP-1 medications like Wegovy and Ozempic can quietly reduce bone mineral density, especially during rapid weight loss phases — and most users are never warned about it.
- Collagen makes up roughly 90% of the organic bone matrix, meaning collagen peptide supplementation is one of the most direct natural strategies to support bone structure during weight loss.
- Postmenopausal women and adults over 50 face the highest risk of GLP-1-related bone loss, but anyone on long-term GLP-1 therapy should be paying attention to bone health markers.
- Fracture risk data for GLP-1 users is still inconclusive — there’s a critical gap in the research that makes proactive bone support even more important right now.
- A combination of collagen peptides, vitamin K2, vitamin D3, magnesium, and weight-bearing exercise represents the most well-rounded natural approach to protecting bones while on GLP-1 medications.
Article-At-A-Glance
GLP-1 medications are changing the weight loss landscape — but what they’re doing to your bones is a conversation that’s long overdue.
Millions of people are now on GLP-1 receptor agonists (GLP-1Ra) like semaglutide (Wegovy, Ozempic) and liraglutide (Saxenda) for weight management. The results on the scale can be dramatic. But underneath that success story, a quieter problem is developing in the skeletal system. Research published between 2013 and 2024 confirms that GLP-1Ra promotes bone remodeling that favors resorption — the process where bone breaks down faster than it rebuilds. For anyone on these medications long term, that’s a serious concern worth addressing head-on. Platforms like Legacy are helping bridge this gap by connecting patients with clinical guidance that goes beyond just the prescription.
GLP-1 Medications Are Quietly Affecting Your Bones
Most people starting a GLP-1 medication are focused on one thing: losing weight. What they’re rarely told is that the same mechanisms driving that weight loss can also accelerate bone turnover in ways that increase long-term fracture risk. The skeletal system is not a passive structure — it’s in constant metabolic conversation with the rest of the body, and significant caloric restriction disrupts that conversation significantly.
Why Rapid Weight Loss From GLP-1s Puts Bone Density at Risk
When body weight drops rapidly, the mechanical load on the skeleton decreases. Bones respond to load — that’s a core principle of bone biology. Less body weight means less daily stress on bones, which signals the body to reduce bone mass accordingly. Combined with the reduced caloric intake that typically accompanies GLP-1 use, the body may also pull minerals and nutrients from bone tissue to meet other metabolic demands. The result is a measurable reduction in bone mineral density (BMD), even in otherwise healthy adults.
What the Latest Research Says About GLP-1Ra and Bone Mineral Density
A comprehensive literature review covering preclinical studies and human data from January 2013 to December 2024 identified consistent patterns in how GLP-1Ra affects bone. The findings are nuanced but clear in one direction: GLP-1Ra causes a modest but real reduction in BMD and shifts bone remodeling toward resorption — the same pattern seen with standard calorie restriction.
Interestingly, preclinical bone cell studies did show that GLP-1Ra could be advantageous for bone health at certain concentrations. Liraglutide in particular appeared to positively influence bone metabolism across multiple animal models. However, those favorable effects on bone mineral density and microarchitecture were noted at concentrations significantly higher than those approved for human obesity treatment. That gap matters enormously when translating lab findings to real-world clinical outcomes.
A 2015 study published in the Journal of Clinical Endocrinology & Metabolism by Iepsen, Lundgren, Hartmann et al. found that GLP-1 receptor agonist treatment increased bone formation and prevented bone loss in weight-reduced obese women — an important data point, but one that doesn’t eliminate the need for active bone protection strategies in the broader GLP-1 user population.
Who Is Most Vulnerable: Postmenopausal Women and Men Over 50
Women over 40, particularly those who are postmenopausal, and men over 50 already face an elevated baseline risk of bone density loss. When you add GLP-1-induced bone resorption on top of age-related and hormonal bone loss, the cumulative effect can accelerate the path toward osteopenia or osteoporosis significantly. These groups aren’t just at higher risk — they’re the population least equipped to absorb additional bone turnover without consequences.
As Dr. Neha Agrawal, Pharm.D., AAHIVP, Director of Clinical Pharmacy Services at Legacy, puts it:
“GLP-1s are only one part of the weight loss equation. Without proper diet and exercise, patients may face complications like osteoporosis or sarcopenia.”
That warning extends directly to bone health monitoring — and to the natural support strategies that can make a measurable difference.
How Bone Metabolism Works During Weight Loss
Bone is a living tissue that undergoes a continuous cycle of breakdown and rebuilding. Understanding this cycle is key to understanding why GLP-1 medications — and weight loss in general — can put bones at risk.
|
Bone Process |
What It Involves |
Impact During Weight Loss |
|---|---|---|
|
Bone Resorption |
Osteoclasts break down old bone tissue |
Increases with caloric restriction and reduced mechanical load |
|
Bone Formation |
Osteoblasts build new bone matrix using collagen and minerals |
Can slow when nutrient availability is limited |
|
Bone Remodeling |
Ongoing balance between resorption and formation |
Shifts toward net bone loss during rapid or prolonged weight reduction |
|
Bone Mineral Density (BMD) |
Concentration of minerals like calcium and phosphate in bone |
Measurably reduced in GLP-1Ra users per 2013–2024 literature review |
What High Turnover Bone Loss Means for GLP-1 Users
High bone turnover isn’t automatically dangerous — it’s a normal part of bone maintenance. But when resorption consistently outpaces formation, the net result is thinner, weaker bone over time. For GLP-1 users experiencing significant weight reduction, this imbalance can develop gradually and silently, often showing no symptoms until a fracture occurs or a DXA scan reveals the damage already done.
How Calorie Restriction Triggers Bone Resorption
GLP-1Ra-induced bone changes closely mirror what happens during standard calorie restriction diets. When caloric intake drops significantly, the body reduces circulating insulin-like growth factor 1 (IGF-1), a key hormone that supports osteoblast activity — the bone-building side of the equation. Simultaneously, cortisol levels can rise during periods of caloric stress, further promoting bone breakdown. This is why bone health during any major weight loss intervention, pharmaceutical or dietary, requires active management rather than a passive approach. For more insights on this topic, check out the benefits of vitamin D for muscle preservation and weight loss.
Early animal research reinforced this connection powerfully. The first evidence of GLP-1’s skeletal role came from GLP-1 receptor knockout (KO) mice, which showed reduced trabecular bone mass due to increased osteoclast activity — directly linking GLP-1 signaling to bone resorption control at the cellular level.
The Difference Between Bariatric Surgery and GLP-1-Induced Bone Changes
Bariatric and metabolic surgery produces well-documented effects on bone — significant weight reduction of approximately 7–10% through surgical intervention consistently results in measurable bone density loss. GLP-1Ra-induced weight loss follows a similar metabolic pattern, though the magnitude and mechanisms may differ. Surgical procedures can also affect nutrient absorption directly (particularly calcium and vitamin D), adding another layer of bone risk not typically present with pharmaceutical GLP-1 therapy alone.
What Collagen Peptides Do for Bone Health
Collagen is not just a skin supplement. It is the primary structural protein in bone, forming the organic scaffolding that minerals like calcium and phosphate anchor to. Without a healthy collagen matrix, even optimal mineral intake cannot produce strong, resilient bone tissue.
This is the piece of bone health that gets overlooked in almost every conversation about calcium, vitamin D, and fracture prevention. Minerals give bone its hardness, but collagen gives it its flexibility and tensile strength — the ability to absorb impact without fracturing. Both components are non-negotiable for functional bone integrity.
The Role of Collagen in Bone Matrix Structure
Approximately 90% of the organic bone matrix is made up of Type I collagen. This dense protein framework is produced by osteoblasts and acts as the template onto which hydroxyapatite crystals (the mineral component of bone) are deposited. When collagen production is compromised — through aging, nutrient deficiency, or accelerated bone turnover — the structural integrity of that mineral lattice is weakened from the inside out.
This is particularly relevant for GLP-1 users because the same caloric and nutrient restriction that slows osteoblast activity also reduces the amino acid availability needed for collagen synthesis. Glycine, proline, and hydroxyproline — the three dominant amino acids in collagen — must be present in sufficient quantities for the body to maintain and repair bone matrix effectively. Collagen peptide supplementation directly addresses this supply gap.
How Collagen Peptides Support Bone Mineral Density
Collagen peptides are hydrolyzed fragments of collagen protein — broken down into smaller chains of amino acids that absorb rapidly through the gut and travel directly to bone tissue. Once there, they stimulate osteoblast activity, promoting new bone matrix formation. They also appear to suppress osteoclast activity, which means they work on both sides of the bone remodeling equation simultaneously — building more while breaking down less. For a deeper understanding of this process, you can explore this scientific article that details the effects of collagen peptides on bone health.
Research supports this dual action. Studies using specific bioactive collagen peptides have demonstrated measurable increases in bone mineral density in postmenopausal women — one of the highest-risk groups for both GLP-1-related and age-related bone loss. The key mechanism appears to be collagen peptide fragments acting as signaling molecules that directly trigger osteoblast proliferation and collagen synthesis within bone tissue itself, not just providing raw amino acid material.
Collagen Peptides vs. Calcium Supplements: Which Matters More for Bone Strength
Calcium gets most of the attention in bone health conversations, but here’s the reality: calcium without an adequate collagen matrix to anchor to is far less effective. Think of it like trying to apply cement to a crumbling wall — the mineral can’t do its job if the structural framework beneath it is compromised. Collagen provides the architecture; calcium provides the hardness. For GLP-1 users experiencing accelerated bone turnover, prioritizing collagen peptide supplementation alongside — not instead of — calcium and vitamin D creates a far more complete bone protection strategy than any single supplement alone.
“Clean Eatz Kitchen” from www.cleaneatzkitchen.com and used with no modifications.
Collagen Peptides as a Natural Support Strategy for GLP-1 Users
GLP-1 medications suppress appetite significantly, which means most users are consuming considerably fewer calories and, by extension, considerably less protein than their body needs to maintain muscle and bone tissue. Collagen peptides offer a highly bioavailable, low-calorie protein source that directly targets the structural needs of bone — making them a uniquely well-suited supplement for this population.
The practical advantage of collagen peptides is their versatility. They dissolve easily in hot or cold liquids, are virtually tasteless, and add meaningful protein grams without triggering the appetite suppression rebound that whole food protein sources sometimes cause in GLP-1 users. For someone eating 1,000 to 1,400 calories per day on a medication like Wegovy or Saxenda, every gram of targeted nutrition counts.
Why GLP-1 Users Have Higher Collagen Needs Than the General Population
The combination of reduced caloric intake, accelerated bone resorption, and lower mechanical load on the skeleton creates a perfect storm of collagen depletion in GLP-1 users. Natural collagen production also declines with age — dropping roughly 1% per year after age 25 — meaning that older adults on GLP-1 medications are dealing with compounding deficits from multiple directions simultaneously.
Several factors make GLP-1 users particularly dependent on external collagen support:
- Reduced total protein intake from appetite suppression limits the raw amino acids available for collagen synthesis
- Accelerated bone remodeling driven by GLP-1Ra increases the demand for new collagen matrix production
- Caloric restriction patterns similar to those seen in GLP-1 therapy are independently linked to decreased bone collagen cross-linking — a marker of bone quality
- Age-related collagen decline compounds the deficit, especially in adults over 40 already on GLP-1 therapy for obesity management
- Reduced mechanical load as body weight decreases signals the body to produce less bone matrix overall, further cutting endogenous collagen production in bone tissue
Addressing this through targeted collagen peptide supplementation isn’t optional for long-term GLP-1 users — it’s one of the most logical and direct interventions available without a prescription.
How to Choose a Pharmaceutical-Grade Collagen Peptide Product
Not all collagen supplements are created equal. For bone-specific benefits, look for products that contain Type I hydrolyzed collagen peptides, ideally derived from bovine or marine sources with third-party testing verification. Clinically studied branded collagen ingredients like FORTIBONE® (a specific bioactive collagen peptide developed by Gelita) have peer-reviewed data specifically on bone mineral density outcomes — which is a meaningful differentiator from generic collagen powders. Effective doses in research settings typically range from 5 grams to 15 grams per day, taken consistently over a minimum of 12 weeks to see measurable bone-relevant changes.
“Clean Eatz Kitchen” from www.cleaneatzkitchen.com and used with no modifications.
Other Natural Remedies That Support Bone Health on GLP-1 Medications
Collagen peptides are the foundation, but bone health is a multi-nutrient equation. Several well-researched natural compounds work synergistically with collagen to protect and rebuild bone density during GLP-1 therapy — and each one addresses a distinct gap in the bone remodeling process.
1. Vitamin K2 and Its Role in Directing Calcium to Bones
Vitamin K2 — specifically in its MK-7 form — activates a protein called osteocalcin, which is responsible for binding calcium to the bone matrix. Without adequate K2, calcium absorbed from food or supplements circulates in the bloodstream rather than integrating into bone tissue. This is why calcium supplementation without K2 has been associated in some research with arterial calcification rather than bone strengthening — the calcium goes somewhere, just not where you want it.
For GLP-1 users, whose reduced food intake may already limit dietary K2 sources like fermented foods, hard cheeses, and grass-fed animal products, supplementation with 90 to 180 micrograms of MK-7 daily is a targeted and evidence-supported strategy to ensure calcium is actually doing its job in bone tissue. For more on the benefits of vitamins, check out this guide on vitamin D benefits.
2. Magnesium for Bone Density Support
Magnesium is involved in over 300 enzymatic reactions in the body, and bone metabolism is directly among them. Approximately 60% of the body’s total magnesium is stored in bone, where it influences the size and stability of hydroxyapatite crystals — the mineral structure that gives bone its hardness. Low magnesium status is independently associated with lower bone mineral density and increased fracture risk, making it a critical co-factor for anyone experiencing accelerated bone turnover. Magnesium glycinate or magnesium malate forms offer superior absorption compared to magnesium oxide, which has notoriously poor bioavailability despite being common in low-cost supplements.
3. Weight-Bearing Exercise to Counter Bone Loss
No supplement stack fully compensates for the mechanical stimulation that bone tissue requires to maintain density. Weight-bearing and resistance exercise creates the physical stress that signals osteoblasts to produce new bone matrix — and for GLP-1 users losing significant body weight, this external mechanical load becomes even more important as the natural load from body weight decreases. For more on maintaining muscle during weight loss, explore the benefits of Vitamin D.
The most effective exercise types for bone preservation during weight loss include a combination of the following:
- Resistance training with free weights or machines targeting major muscle groups at least 2–3 times per week
- High-impact activities like walking, hiking, or jogging that load the hip and spine — the two sites most vulnerable to osteoporotic fractures
- Balance and stability training to reduce fall risk, which becomes more relevant as muscle mass (and body weight) decreases on GLP-1 therapy
- Progressive overload — gradually increasing resistance over time to continue stimulating bone adaptation rather than plateauing
Even 20 to 30 minutes of structured resistance training three times per week produces measurable benefits for bone mineral density over a 6–12 month period, making it one of the highest-return natural interventions available to GLP-1 users.
4. Vitamin D3 for Calcium Absorption
Vitamin D3 is the essential gateway nutrient for calcium absorption in the gut — without sufficient D3, the body absorbs as little as 10–15% of dietary calcium compared to 30–40% when D3 status is optimal. For GLP-1 users eating reduced food volumes, the stakes of vitamin D deficiency are especially high. A daily dose of 1,000 to 2,000 IU of vitamin D3, combined with vitamin K2 to direct that calcium appropriately, forms the mineral absorption backbone of any serious bone protection protocol for people on GLP-1 medications.
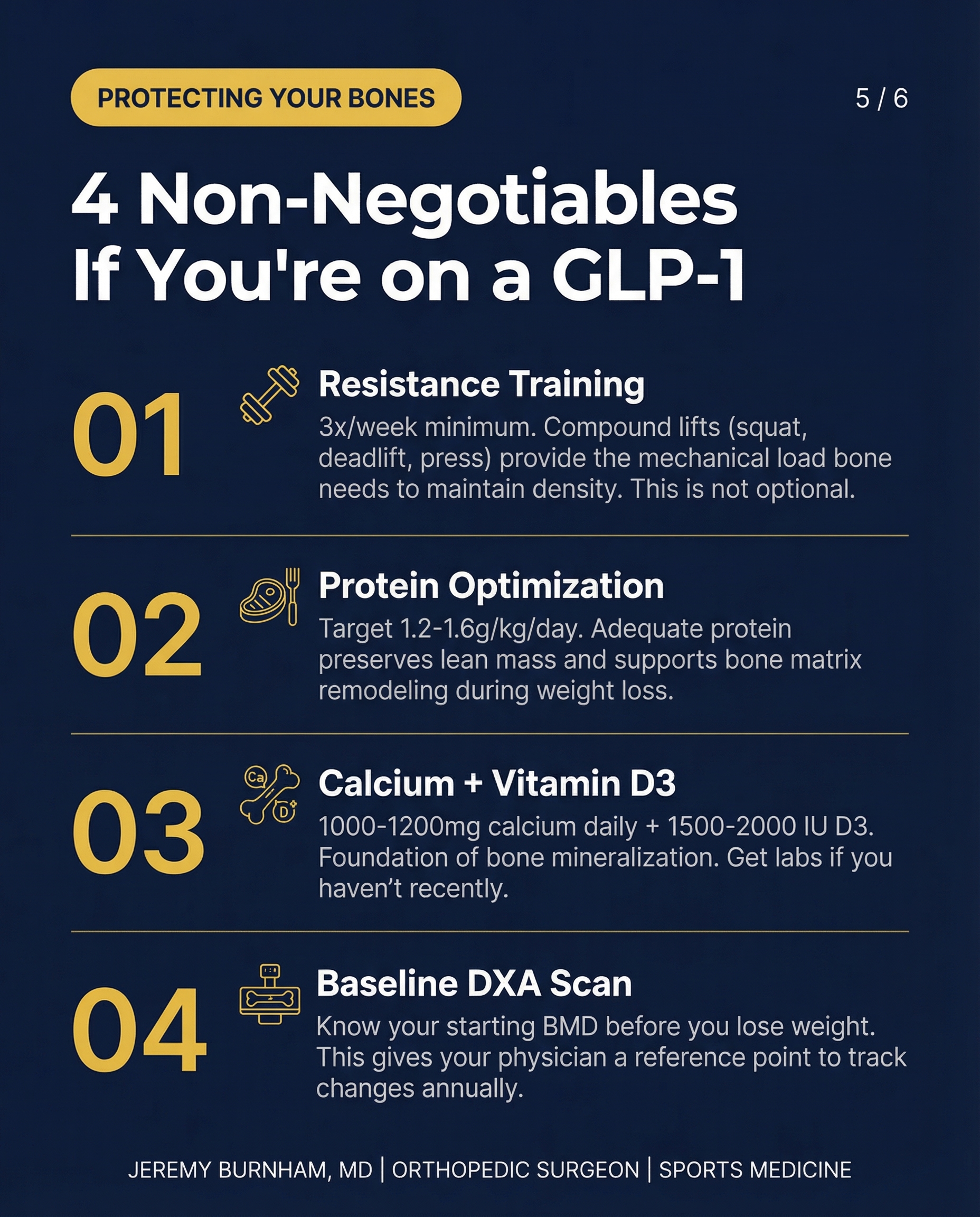
“GLP-1s and Bone Health: The Hidden …” from www.jeremyburnhammd.com and used with no modifications.
What Still Needs to Be Proven: Gaps in GLP-1 and Bone Research
The science on GLP-1 medications and bone health is moving fast, but it still has significant blind spots. What the research confirms so far is directional — GLP-1Ra shifts bone remodeling toward resorption, reduces BMD modestly, and mirrors the skeletal effects of calorie restriction. What it hasn’t yet answered is arguably more important for the millions of people currently on these medications: does that bone density reduction actually translate into a meaningfully higher fracture rate, and over what time horizon? For those interested in related topics, the benefits of Vitamin D for muscle preservation and weight loss may also be worth exploring.
Why Fracture Risk Data for GLP-1Ra Users Remains Inconclusive
The comprehensive literature review covering 2013 to 2024 was explicit on this point — fracture risk associated with GLP-1Ra versus controls with obesity undergoing surgical or non-surgical weight loss procedures has not been adequately studied. Bone mineral density is a proxy measurement. It correlates with fracture risk but doesn’t determine it absolutely. Bone quality — including collagen matrix integrity, trabecular architecture, and mineralization patterns — matters just as much as raw density numbers. Until long-term fracture outcome data exists specifically for GLP-1Ra users, clinicians and patients are making bone health decisions without a complete picture. That uncertainty alone is a compelling reason to act proactively rather than wait for the research to catch up.
The Need for Long-Term Bone Health Monitoring in GLP-1 Patients
Current clinical practice does not universally mandate baseline or follow-up bone density scanning for patients starting GLP-1 therapy. That gap is a problem. A DXA (dual-energy X-ray absorptiometry) scan provides a baseline measurement of bone mineral density at the hip and lumbar spine — the two fracture sites most clinically significant for adults. Without that baseline, any deterioration happening during GLP-1 treatment is essentially invisible until it reaches a threshold that produces symptoms or a fracture event.
The recommendation from bone health experts is clear and practical: anyone starting long-term GLP-1 therapy — particularly women over 40, postmenopausal women, men over 50, and anyone with a prior history of low bone density — should request a baseline DXA scan and schedule follow-up monitoring annually or biannually. Combining that monitoring with proactive natural supplementation strategies creates the most defensible approach to protecting skeletal health during what can be a transformative but metabolically demanding period of weight loss.
Protecting Your Bones While on GLP-1 Medications Starts Now
The window for meaningful bone protection is open right now — not after years of GLP-1 therapy have passed. Bone loss that accumulates over 12 to 24 months on a GLP-1 medication without countermeasures is far harder to reverse than it is to prevent. The natural remedy framework outlined in this article — collagen peptides, vitamin K2, vitamin D3, magnesium, and structured weight-bearing exercise — isn’t speculative. Each component addresses a documented mechanism of GLP-1-associated bone risk with real physiological logic behind it.
Start with a baseline DXA scan, implement a collagen peptide protocol of 10 to 15 grams daily, optimize your vitamin D3 and K2 levels, ensure adequate magnesium intake, and build resistance training into your weekly routine. These aren’t heroic interventions — they’re foundational steps that compound significantly over time. The combination of pharmaceutical weight management and targeted natural bone support isn’t a contradiction; it’s the most complete and intelligent approach to long-term health on GLP-1 therapy.
Frequently Asked Questions
Do GLP-1 medications like Wegovy and Saxenda cause bone loss?
GLP-1 medications like Wegovy (semaglutide) and Saxenda (liraglutide) are associated with a modest but measurable reduction in bone mineral density, according to a comprehensive literature review covering 2013 to 2024. They promote bone remodeling that favors resorption — meaning bone breaks down slightly faster than it rebuilds — a pattern similar to standard calorie restriction. Whether this translates directly into increased fracture risk remains under investigation, but the bone density changes are real and warrant active monitoring and supplementation.
How much collagen should I take daily if I am on a GLP-1 medication?
Research on bone-specific collagen peptide supplementation typically uses doses between 5 and 15 grams per day, taken consistently over a minimum of 12 weeks to produce measurable effects on bone markers. For GLP-1 users dealing with reduced total protein intake and accelerated bone turnover, targeting the higher end of that range — around 10 to 15 grams of hydrolyzed Type I collagen peptides daily — is a well-supported starting point. Look for products featuring clinically studied bioactive collagen peptides like FORTIBONE® with third-party testing verification rather than generic collagen powders.
Can collagen peptides reduce fracture risk for GLP-1 users?
Collagen peptides support bone health by stimulating osteoblast activity (bone building) and suppressing osteoclast activity (bone breakdown), while directly supplying the amino acids needed to maintain and repair the bone collagen matrix. Since collagen makes up approximately 90% of the organic bone matrix, adequate collagen peptide supplementation addresses a foundational gap in bone quality — not just density. While direct fracture outcome studies in GLP-1 users specifically are still lacking, the mechanistic case for collagen peptides as a bone-protective natural remedy in this population is strong and well-grounded in bone biology research.
Are there natural supplements that work alongside collagen to protect bones during weight loss?
Several well-researched natural compounds complement collagen peptides effectively for bone protection during GLP-1 therapy. Vitamin D3 (1,000 to 2,000 IU daily) optimizes calcium absorption in the gut. Vitamin K2 in MK-7 form (90 to 180 micrograms daily) activates osteocalcin to direct that absorbed calcium into bone tissue rather than soft tissue. Magnesium glycinate or malate supports the crystalline mineral structure of bone and is often deficient in adults eating reduced-calorie diets.
Together, these four nutrients — collagen peptides, vitamin D3, vitamin K2, and magnesium — form an evidence-based natural stack that targets every major mechanism of GLP-1-associated bone loss. Adding structured weight-bearing and resistance exercise completes the protocol by providing the mechanical stimulus that no supplement alone can replicate. This combination represents the most comprehensive non-prescription bone protection strategy currently available to GLP-1 users.
Should I get a bone density scan if I am taking a GLP-1 medication long term?
Yes — a baseline DXA scan is strongly advisable for anyone planning long-term GLP-1 therapy, particularly those in higher-risk categories: women over 40, postmenopausal women, men over 50, and individuals with a personal or family history of osteoporosis or low bone density. A DXA scan measures bone mineral density at the hip and lumbar spine — the sites most clinically significant for fracture risk — and provides the baseline needed to detect any deterioration during treatment.
Without a starting measurement, there is no way to know whether bone density is declining during GLP-1 therapy until the loss is severe enough to produce symptoms or a fracture. Annual or biannual follow-up scans are a reasonable monitoring frequency for long-term GLP-1 users, and the results should inform both medical management decisions and the intensity of natural supplementation protocols.